What are the levels of E M service based on?
.
Herein, what are the 4 levels of history in E&M coding?
The four recognized levels of history are problem-focused, expanded problem-focused, detailed, and comprehensive. The number of elements documented in the progress note determines level selection.
Similarly, how is EM level calculated? Three components determine the appropriate billing level for an e/m visit: history, examination, and medical decision-making. Each of these, in turn, has various levels of complexity and sub-components.
Additionally, what are the 3 key components of EM services?
The three key components of E&M services, history, examination, and medical decision making appear in the descriptors for office and other outpatient services, hospital observation services, hospital inpatient services, consultations, emergency department services, nursing facility services, domiciliary care services,
What are EM codes?
Evaluation and management coding (commonly known as E/M coding or E&M coding) is a medical coding process in support of medical billing. This allows medical service providers to document and bill for reimbursement for services provided.
Related Question AnswersWhat are the four elements of history?
Science Lesson: Earth, Water, Air, and Fire. The ancient Greeks believed that there were four elements that everything was made up of: earth, water, air, and fire. This theory was suggested around 450 BC, and it was later supported and added to by Aristotle.What are the 8 elements of HPI?
CPT guidelines recognize the following eight components of the HPI:- Location. What is the site of the problem?
- Quality. What is the nature of the pain?
- Severity.
- Duration.
- Timing.
- Context.
- Modifying factors.
- Associated signs and symptoms.
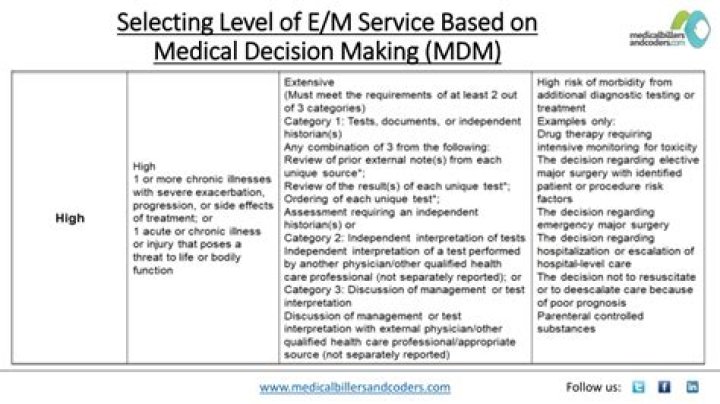
How is MDM level calculated?
Each of the three MDM areas should be scored. The level is determined by selecting the highest two of the three distinct areas.There are four levels of MDM to support the five ED E/M codes:
- Straight forward (99281)
- Low (99282)
- Moderate (99283 and 99284)
- High (99285)
What is the difference between the 1995 and 1997 guidelines?
Applying guidelines For example, the 1997 guidelines allow consideration of chronic or inactive conditions in the review of systems and history, whereas the 1995 guidelines only count comorbidities.What is a detailed interval history?
Answer: It is a history that does not require past medical, family, or social history. An interval history is needed for a subsequent hospital visit or subsequent nursing facility visit. CPT® wording is, “an interval expanded focused history” or “an interval detailed history,” depending on the level of visit.What is a detailed history?
The Detailed History is the second highest level of history and requires a chief complaint, an extended HPI (four HPI elements OR the status of three chronic or inactive problems - if using the 1997 E/M guidelines), plus TWO to NINE ROS, plus at least ONE pertinent element of PFSH .What is a complete review of systems?
The Review of Systems (ROS) is an inventory of specific body systems performed by the physician in the process of taking a history from the patient. The ROS is designed to bring out clinical symptoms which the patient may have overlooked or forgotten.What constitutes a detailed exam?
Detailed – an extended examination of the affected body area(s) and other symptomatic or related organ system(s). Comprehensive – a general multi-system examination or complete examination of a single organ system. For purposes of examination, the following body areas are recognized: Head, including the face.What is an e m code and what does it report?
E/M stands for “evaluation and management”. E/M coding is the process by which physician-patient encounters are translated into five digit CPT codes to facilitate billing. CPT stands for “current procedural terminology.” These are the numeric codes which are submitted to insurers for payment.What is an E&M visit?
One term that is commonly used is E&M visit, which is short form for Evaluation and Management Encounter. The Current Procedural Terminology (CPT) codes cover evaluation and management ( E&M) services, which clinicians use in billing for office and hospital visits.How do you improve em coding?
Below are six ways to improve coding and compliance that will increase revenue:- Designate an in-house claims tracker.
- View denials as a learning experience.
- Bring physicians and others on board with coding.
- Keep current on coding regulations and resources.
- Read provider or clinician notes fully before coding.